
Psycodex #5: Anxiety
Comorbidity, Anxiety & Obsessions, and the briefest summary of psychology ever.

This is the fifth post in a series of weekly primers on what Australian medical students learn in psychiatry. “/” indicates content taught within the medical curriculum; “\” indicates content beyond. Past posts: Introduction, #1 Depression, #2 Mania, #3 Psychosis, #4 Addiction.
\ The more I unravel the tapestry of psychiatry, the more I find myself curiously confused.
Take anxiety, for instance. For the less initiated, one may think this to be quite distinct from constructs like depression or obsessive compulsions.
But the saying goes; comorbidity is the rule, not the exception. These concepts are both very heterogeneous (many different types), and difficult to separate from each other. For instance, an estimated 40-70% of people with an anxiety disorder have comorbid depressive disorder, and up to 75.8% of those with OCD have some comorbid anxiety disorder. The error bars are large, but there’s clearly significant overlap.
This is partly explained by the construct itself. After all, consider that the DSM-V criteria of both Major Depressive Disorder and Generalised Anxiety Disorder share common symptoms (issues with sleep, energy, and concentration). These seem to act as just markers of dysfunction, rather than key elements which carve apart the diagnostic categories.
Further, there are transdiagnostic markers which aren’t captured by the DSM itself which may underlie comorbidities. Take rumination, referring to the repetitive dwelling on negative feelings and past events. This has been proposed both as an example of a transdiagnostic factor that leads to MDD or GAD - thus accounting for the comorbidity - and as a key target in therapies, such as mindfulness, rumination-focused CBT, and even neurofeedback.
Biological psychiatry hopes to then further account for such transdiagnostic constructs through neuroimaging and electrophysiological tools - developing models of transdiagnostic biotypes which hope to both be predictive of concepts like rumination and thus treatment outcome.
Regardless, until this research is borne out and a new paradigm is ushered in, there is utility in understanding humanity’s current attempts at carving out these concepts, and how this relates to existing treatments. The below presents what a 7-week term in psychiatry has to offer.
/ So, You Think You’re Clinically Anxious (and Obsessive)
Anxiety is defined in the DSM as “anticipation of future threat”, which then leads to cognitive, physiological, and behavioural responses.
There are plenty of evolutionary theories of the utility of normal anxiety to help us avoid future threats, acting as a warning signal for the mind. It is a disorder when this warning signal is overactive, creating distress and stopping us from engaging in society.
To briefly describe some of the most common DSM anxiety disorders -
Generalised Anxiety Disorder: GAD is an >6mth encompassing anxiety which is related to several domains (such as work, school, relationships). GAD symptoms are memorised with the mnemonic WATCHERS, where Worry and Anxiety are present, and at least 3 of Tension, Concentration difficulty, Hyperarousal, Energy loss, Restlessness, and Sleep disturbance.
Social Anxiety Disorder: SAD is a >6mth fear/anxiety of social situations that can lead to scrutiny. These situations consistently provoke these symptoms, actively avoided, and out of proportion in the sociocultural context.
Agoraphobia: AG is a >6mth fear/anxiety of being in public locations due to fear of panic-like symptoms or embarrassment, leading to avoidance.
Panic Disorder: PD is characterised by: 1) recurrent panic attacks, 2) the worry of these panic attacks. Panic attacks are described as an abrupt surge of fear, which can have physiological manifestations (ie palpitations, sweating, trembling, chest pain), and psychological (i.e. fear of losing control, dying, derealisation, depersonalisation). Post-attacks, PD has persistent (>1mth) concerns about having another attack, potentially causing avoidant behavioural changes.
Specific Phobia: Specific phobias are as they sound - >6mth significant fear/anxiety provoked by a particular situation (ie heights, spiders, blood) and causes avoidance.
Obsessive-Compulsive Disorders were previously characterised under anxiety disorders in the DSM-IV, but they have been separated in the DSM-V in light of distinct phenomenology, purported neurobiological mechanisms, and treatment response patterns.
OCD involves the presence of obsessions, compulsions, or both - which is significantly time-consuming (ie >1hr) and causes distress. Obsessions are defined by recurrent, uncontrollable, persistent thoughts and urges, which are often ego-dystonic and cause anxiety. Compulsions are repetitive behaviours that attempt to soothe these anxieties, but are not logically connected.
For instance, obsessions can be related to doubt, symmetry, harming others, sex, safety. Compulsions include checking things, arranging objects, counting, or mental thoughts.
I have a friend who struggles with harm-related obsessions. These intrusive thoughts are experienced as ego-dystonic and distressing; and lead to avoidant behaviours. He shared with me a poem he wrote on an early winter’s day, which helped him relieve these distressing thoughts:
The feeling gnaws at me, just below the surface During these grim winter days, thought without purpose It screams for release, boring just below your skin An answer to all of my accumulated sins. But I know the feeling is but another lie And that your yearned-for release will never appease And these many twisted promises of comfort Act as nothing more than a malicious tease. Nothing more than shallow hopes to fulfill The shallow desires of a shallow man And I fear that to cut too deep risk damage To the edge of your oh-so precious soul’s span. But the thought is ever so potent And the tools for action are all here And the ease of release tempts me To grasp onto that which is dear.
Other OCD-related DSM diagnoses include -
Body Dysmorphic Disorder: Preoccupation with defects in physical appearance, with repetitive behaviours related to appearance. This includes muscle dysmorphia, which is specific to muscle bulk.
Hoarding Disorder: Difficulty discarding items.
Trichotillomania: Recurrent hair-pulling, and attempts to stop.
Excoriation Disorder: Recurrent skin-picking, and attempts to stop.
/ Oversimplified Psychology and Medications
The management for anxiety-related disorders in psychiatric guidelines always encourages psychology first-line. When these don’t work, or are too expensive/inconvenient, we turn to medications. Here, we will discuss a quick overview of both.
A brief walk through the history of psychology leads us to three predominant schools of thought.
Psychodynamic (1890s-) - Freud & Jung created the talking therapy in the search for how unconscious conflicts drove behaviour, linking early childhood experiences and maladaptive defenses to existing anxieties. Although still relevant in attachment and personality, this form of therapy is less used in the context of anxiety and obsessions.
Behavioural (1900s-1950s): Pavlov (of Pavlov’s Dog fame) and Skinner were the foundational behaviourists who posited that another element of the unconscious included learned associations. In this framework, fears develop from classical conditioning (ie being bitten by a dog associates all future dogs with pain), and the resultant anxiety is maintained by operant conditioning (ie behaviours that reduce anxiety are negatively reinforced).
This is the motivating framework behind the modern tool for Exposure and Response Prevention (ERP) therapy which is used first-line in OCD and some anxiety disorders.
Cognitive (1960s-): Beck is credited with establishing the connection between emotion, cognition, and behaviour; with the goal of Cognitive-Behavioural Therapy then to adjust cognition to reduce unwanted behaviours. In anxiety, this manifests as distorted cognitions, such as catastrophising (assuming worse cases), overestimation of threat, or uncertainty intolerance.
CBT is considered the most evidence-based therapy (perhaps related to being most amenable to scientific study), and used particularly in anxiety and depression.
Medications appear to work differentially for the clinical disorders - with a rough hierarchy of efficacy being PD > GAD > SAD, and OCD being the least amenable to medication. These medications are summarised in this table:
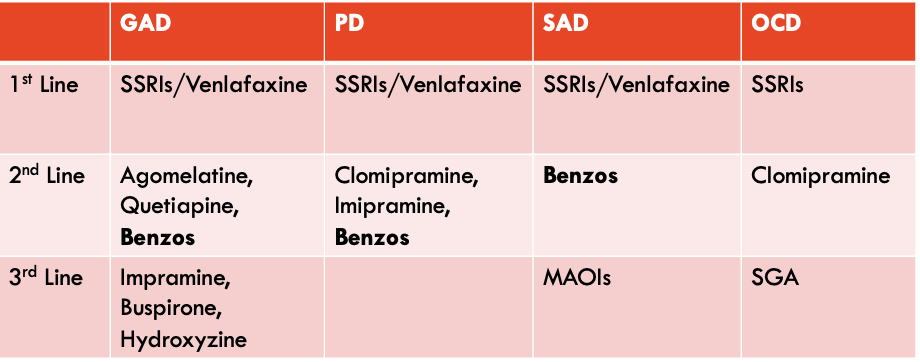
The 1st line for most anxiety disorders are SSRIs, the antidepressant class as described in #1 Depression. Venlafaxine, an Serotonin-Noradrenaline Reuptake Inhibitor, is used as an alternate option with similar tolerability. The mechanism? Probably related to reducing neuroticism, reducing negative emotional processing, and some emotional blunting.
Benzodiazepines are common as the second line for most anxiety disorders; they increase GABA action by attaching to the GABA-A receptor, and increase the frequency of channel opening. This class is well known for its rapid onset of sedative action, relieving anxious symptoms in minutes. They are the same ones used in drug detox (as discussed in #4 Addiction), and have risks of dependence and withdrawal symptoms.
The other medications are a mix of classes, from tricyclic antidepressants (Imipramine, Clomipramine), second generation antipsychotics (ie Quetiapine), and some specific third line drugs in GAD such as buspirone (known as a ‘Spiro’ drug) and hydroxyzine (an anti-histamine).
The OCD-related disorders all include SSRIs as their medication of choice first-line. Interestingly, the disorders related to obsessions around picking at the body (trichotillomania, Excoriation Disorder) also have N-Acetylcysteine indicated; the same medication used in paracetamol overdose by binding to the toxic metabolite NAPQI. The hypothesised mechanism in OCD is related to its glutamatergic action, but this is poorly understood.
\ These are the medical solutions to anxiety. But the modern world is filled with abundant products for avoidance and self-soothing - Alcohol, drugs, TV, social media, video games... Although still debated, the glaring role of technology in The Anxious Generation feels obvious. Medicine and psychology only represent the modern incarnation of anxiety management - but the age old remedies of philosophy, performance, and prayer will always persist.
P.S. I’d love to hear what you found interesting, and what you’d like more of in the comments.